You launched your remote patient monitoring program with real hope. The devices arrived, the patients enrolled, and the revenue potential looked great on paper. Then reality hit. Your staff was already stretched thin, the data never stopped coming in, and little by little the whole thing started falling apart. If that sounds familiar, you are not alone. Across Texas and the rest of the US, virtual assistants are now the reason RPM programs survive.
KEY TAKEAWAYS:
- 64% of RPM programs fail in year one due to staffing issues, not technology
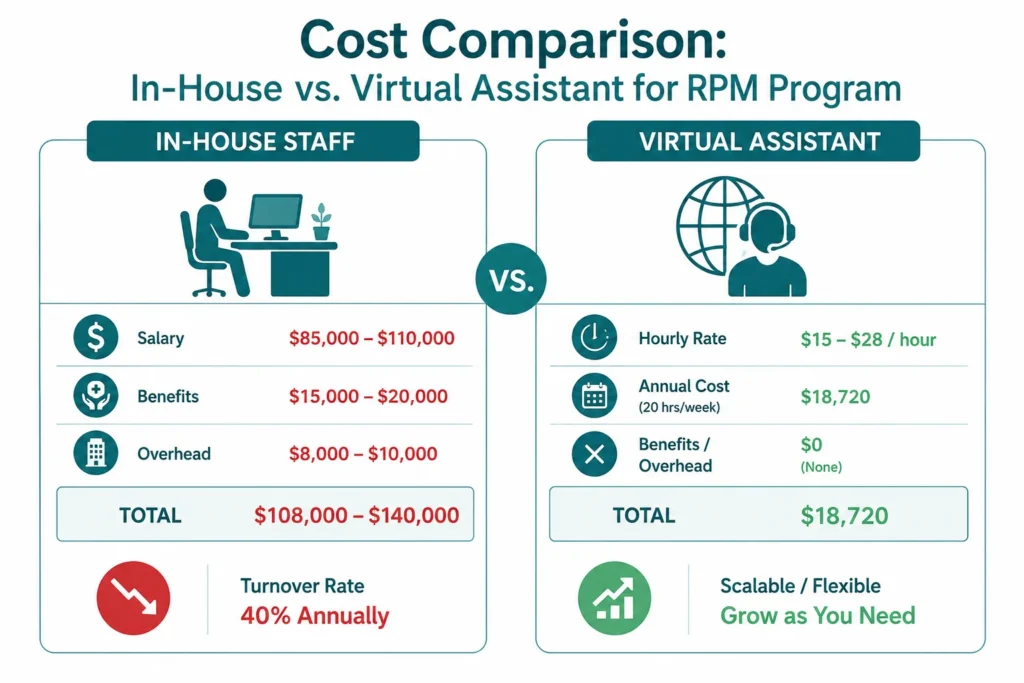
- Virtual assistants cost $15-28/hour vs. $85-110K annually for in-house coordinators
- A 50-patient RPM program generates $48,000 yearly but requires 53 hours of weekly staff time
- VA-supported programs deliver equivalent outcomes with better documentation and fewer missed alerts
- Most practices reach profitability within 3-6 months after implementing virtual assistant support
The Numbers Behind the Problem
Sixty-four percent of RPM programs close within their first year. The reason is almost never technology. It is the people, or rather the lack of them. Managing remote patient monitoring services for just 100 enrolled patients requires 53 hours of staff time every single week. That is more than a full-time job dedicated to one program.
The financial hit is real: the average practice walks away from $150,000 in annual revenue because the program never gets properly managed. For a 50-patient program, that is $75,000 to $100,000 in untouched billing sitting right there, while 73 percent of documentation goes incomplete.
And the patients? Sixty-two percent drop out within six months when nobody is consistently following up. That is not a technology failure. That is a staffing failure.
Why Hiring In-House Does Not Solve It
A qualified care coordinator in Texas costs between $85,000 and $110,000 a year when you factor in salary, benefits, and overhead. For a 50-patient RPM program generating around $48,000 annually, the math just does not work. You end up losing money before the physician even spends a minute reviewing the data.
There is also the turnover problem. Roles built around repetitive monitoring tasks see roughly 40 percent annual turnover. You hire, train for three to six months, and then start over. Meanwhile your remote patient monitoring rpm program stalls every time a key person leaves.
The real cost of doing nothing: your competitors in Dallas, Fort Worth, and across DFW are already figuring this out. The practices that crack the staffing problem now will own this market in two years.
What a Healthcare Virtual Assistant Actually Does
A healthcare virtual assistant for RPM is not a call center agent reading from a script. These are trained remote professionals with medical backgrounds who handle the daily work that keeps your program alive. Think of them as your dedicated care coordination team working remotely on your schedule.
Their day looks something like this: morning starts with reviewing overnight alerts and flagging anything that needs clinical attention. Then they work through scheduled patient outreach calls, troubleshoot device issues, and close out the day with documentation that meets Medicare billing requirements. All of it done without pulling your in-house staff away from in-person patient care.
For continuous patient monitoring programs specifically, this matters enormously. Physiological monitoring data comes in around the clock. Someone needs to watch it. A virtual medical assistant dedicated to your program means nothing slips through.
The Revenue Math When You Use Virtual Assistants
Here is where it gets interesting. A VA handling your 50-patient RPM program costs around $18,720 a year at 20 hours weekly. Your remote patient monitoring services for those same 50 patients brings in $48,000 annually. That is a net profit of $29,280 before physician time, compared to a $7,000 net loss using in-house staff.
Scale to 100 patients and the difference is even sharper. Traditional staffing gets you roughly break even. With a virtual assistant in healthcare, you are looking at $58,560 in net profit from the same patient volume. That is not a small difference. It changes whether the program exists at all.
Healthcare workflow automation through VA-supported RPM also means cleaner documentation, fewer missed billing thresholds, and more claims that actually get paid on the first submission.
Real Texas Practices, Real Results
A Family Practice in Wylie, TX
Four physicians launched a CHF remote patient monitoring program with 15 patients. Within three months, 67 percent had dropped out. The practice was generating $8,000 a year from the program while spending more in staff overtime.
They brought in a single RPM-specialized virtual medical assistant for 10 hours weekly. Six months later, enrollment grew to 45 patients, the dropout rate fell to 18 percent, and annual RPM revenue hit $43,200. The VA cost $9,360 a year. Net profit: $33,840. The physician’s exact words were: finally profitable without staff burnout.
A Cardiology Practice in Dallas, TX
Eight cardiologists wanted to launch post-discharge remote patient monitoring for 100+ high-risk cardiac patients. They could not justify two full-time coordinators. They built a team of three VAs providing 120 hours of weekly coverage including evenings and weekends.
After 12 months: 112 patients enrolled, hospital readmissions down 38 percent, $134,400 in annual RPM revenue, and $62,400 in avoided readmission penalties. Reducing hospital readmissions alone justified the entire program cost. Total benefit: $196,800. VA cost: $112,320. Net benefit: $84,480.
A Diabetes Clinic in Fort Worth, TX
Sixty patients on continuous glucose monitors but only 40 percent were actually transmitting data. The practice brought in two VAs with diabetes education backgrounds for diabetes remote patient monitoring support. Nine months later, active transmission reached 87 percent, average HbA1c improved by 1.2 percent, and hypoglycemic events dropped 44 percent. Patient satisfaction went from 71 to 94 percent.
How to Get Your RPM Program Running in 30 Days
Week One: Find the Right VA Partner
Start by identifying 3 to 5 specialized healthcare VA agencies. You want someone with prior remote patient monitoring experience, HIPAA training, familiarity with your EHR, and strong patient communication skills. For practices in DFW with large Hispanic patient populations, bilingual VAs add real value for improving patient experience and engagement.
Expect to pay $15 to $28 per hour depending on the agency and the VA’s clinical background. That is still 40 to 60 percent less than in-house staff when you remove benefits and overhead from the equation.
For a trusted resource on RPM standards, the
Centers for Medicare and Medicaid Services RPM billing guidance is worth reviewing before you finalize your protocols.
Week Two: Build Your Protocols
Critical alerts go to the physician immediately: blood pressure above 180/110, oxygen saturation below 90 percent, blood glucose below 70 or above 400. Moderate alerts go to RN review within two hours. Routine follow-up, patient education, medication reminders, and device troubleshooting all go to the VA. This structure keeps clinical staff focused on decisions while the VA handles the volume.
Patient data management becomes simple when everyone knows their lane. The VA tracks time for billing compliance, flags when patients are approaching monthly thresholds, and generates documentation your billing team can actually use.
Weeks Three and Four: Enroll and Launch
Start with 15 to 25 patients. Use the first month to refine protocols based on what actually happens, not what you planned for. Daily check-ins with your VA during the first two weeks catch problems early. By week four, you have real data on alert frequency, patient responsiveness, and documentation quality. From there, you scale with confidence.
The American Medical Association RPM implementation playbook is a solid external reference for protocol development, especially around telehealth virtual assistant integration and escalation pathways.
For practices already navigating referral workflows, our guide on
how missed referrals quietly drain practice revenue covers the front-end gaps that compound RPM billing problems.
What Makes VA-Supported RPM Actually Work Long Term
Patient engagement tools only work when someone is using them consistently. The practices that see the best outcomes from remote health monitoring are the ones that treat the VA relationship like any other clinical role. Weekly supervision calls, monthly chart audits, outcome tracking, and regular protocol updates.
Personalized patient care is not a buzzword here. It is the difference between a patient who stays enrolled for a year and one who stops transmitting data in month two. When your VA remembers that a patient’s granddaughter just started college, or that they finally hit their weight goal last week, the patient feels seen. That is what keeps people engaged in digital patient care programs long term.
Telemedicine support through VAs also extends your practice’s reach beyond the clinic walls. Patients in suburban and rural parts of DFW who cannot easily make it in for regular visits stay connected through consistent remote contact. That improves outcomes and reduces the kind of avoidable hospitalizations that hurt both patients and practices under value-based contracts.

It means every touchpoint a patient has with your practice feels easy, clear, and respectful of their time. Shorter wait times, better communication, and fewer administrative headaches all add up to patients who stay, refer others, and show up to their appointments.
They are the tools that replace the manual, paper-heavy, phone-tag-heavy parts of running a practice. Appointment reminders, online scheduling, digital intake forms, and automated follow-ups all fall into this category. The goal is less friction for patients and less manual work for your staff.
They come in, look at where your practice is losing time and money, and build systems that run those processes automatically. Integrate Point works specifically with healthcare practices to streamline referral tracking, billing workflows, and patient communication so your team can focus on care instead of paperwork.
It is a digital tool that handles patient interactions remotely, scheduling, answering common questions, and sending reminders, without your front desk staff having to do it manually.
They are the systems that keep patients connected to your practice between visits, through automated messages, health reminders, satisfaction surveys, and easy online communication that builds trust and reduces no-shows.
The Honest Reason Most Practices Wait Too Long
Many practices delay RPM because they question remote monitoring quality or worry about compliance. In reality, VAs don’t replace clinical judgment; they manage routine monitoring, documentation, and follow-ups, so providers can focus on patients who need direct care. Remote workflows also create clear audit trails, improving accountability and consistency.
Every month of delay can mean thousands of missed RPM revenue while patients lose valuable support for chronic conditions like diabetes, hypertension, CHF, and COPD.
With Integrate Point, you can launch a secure, compliant RPM program quickly improving patient outcomes while maximizing your practice’s efficiency and revenue.